





Exclusive Stories!
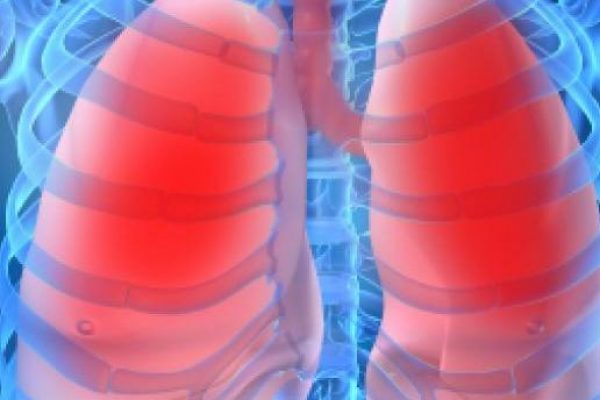
Enjoying the Summer With COPD

Common seasonal activities such as basking in the sun, biking or barbecues can be difficult for those who have difficulty breathing. Outdoor activities can bring serious problems for people with chronic obstructive pulmonary disease (COPD) which is an umbrella term for long term conditions including chronic asthma, bronchitis and emphysema. The simplest outdoors activities can bring on a COPD flare up. (more…)
21st Century Nicotine Maladies Versus Ancient Smoking
(Nicotine Part II)
When I stumbled upon the research conducted by Hermann Niemeyer from the University of Chile in Santiago about pre-hispanic societies consumption of nicotine, I was at first stunned.
Let me explain: (more…)
Choosing the Way You Die

How would you like to die?
Would you like to die rich, fighting for every breath while tethered to every conceivable life support system in the medical world? You are surrounded by lawyers, accountants, relatives, and heck, even distant relatives wishing that you would either pass or not. Or would you like to die a poor man, with not a single cent to your name, with only four or five family members attending your funeral? The cheap white casket gleams with the 15 watt fluorescent bulb at the sides, while daisies and mums adorn your surroundings. Guests are served $10 biscuits.
Danny, don't write about this, nobody in the nine hells cares or wishes to read something negative, something utterly dark and forlorn, something that most people would rather like to delude themselves about or pretend to not exist. As I prevent my fingers from doing their dreary dance on the keyboard, I am reminded that the whole point of trying to quit smoking is to try and stop myself from dying. Every puff, every breath, and every stick is a dreary number deducted from the total I will have. Be it thirty-two years, forty, fifty or god forbid 90 years, I am going to die one day. With smoking, that death becomes more painful for me and my family. But open your mind and think about this for a while: who really knows how they're going to die or when?
Save for those who end their lives prematurely, nobody does. It is something beyond our control even with the most stringent of measures applied. Even legendary visionaries in the known world have no control over this phenomenon of mortality. How did Steve Jobs die? Pancreatic cancer. Did he have the means to prevent it? Maybe yes, maybe no. He certainly had the wherewithal to make the event at least comfortable. There are no accounts to indicate that he was a smoker, drinker, or that he suffered from any other terminal addictions. Some even say he was a fruitarian. But he did die of the dreaded disease nonetheless. The argument is weak, I know. And if we put science into the equation, we know that it's just a matter of statistical probability. Our circumstances, habits, environment and genes all play a role in something that we cannot really factor in. At least, not just yet.
So why should we stop smoking if we are going to die nonetheless?
More Women Found to Have COPD

For the more than 12 million people who suffer from chronic obstructive pulmonary disease or COPD it is poorly understood. It is several ailments that are characterized by airflow obstructions which includes emphysema, chronic asthmatic bronchitis and chronic bronchitis. Many who have COPD don't even know it.
According to the National Heart, Lung and Blood Institute(NHLBI) these respitory diseases are the fourth leading cause of death after heart disease, cancer and strokes. COPD symptoms are very much like viral respiratory illnesses but if wheezing, shortness of breath, chest tightness, and coughing that produces mucus are being suffered by you seeing your doctor is very important for early treatment is key in managing COPD effectively.
Unfortunately there is no cure for COPD but there are medications that will dilate airways and reduce inflammation and exercises to lessen symptoms and strenghthen the lungs.
More women are smoking now days and more women are being found to have the disease. They decline faster than men. And women that smoke the same amount as men are more likely to have greater loss in lung function. This is probably because women's lungs are usually smaller than men's.
Usually COPD is more common in seniors but if they smoke people younger than 65 can develope the disease. A person who started smoking in their teens can develope shortness of breath and wheezing in their 30's or 40's. There may be the early signs of bronchitis or emphazema in the lungs even before the signs of COPD become apparent. For common cancers and heart disease death rates are actually going down but the rates for COPD sufferers are going up. With proper medications and treatments people with COPD can do pretty well but others can develope heart disease and death from respiratory failure. COPD is now the leading cause of death in the U.S.
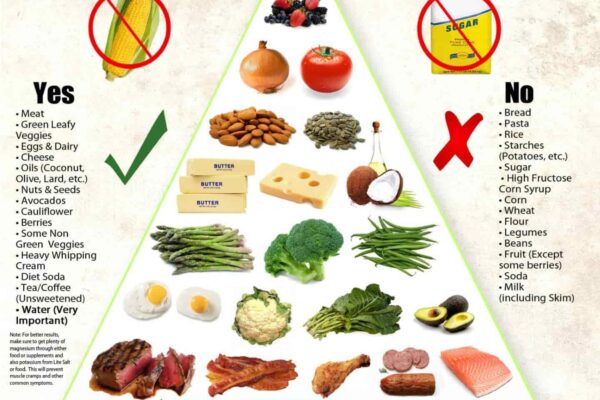
The life expectancy of a COPD patient can improve drastically if they give up smoking, change their lifestyle, take up a healthy diet, take medication and get on a exercise program. There is less strain on the lungs if the patient also loses some weight. If the patient stops smoking they will prevent more damage to the lungs and they start breathing better.
Ninety percent of COPD patients are smokers. Quitting will make a difference even if the patient has smoked for many years. COPD patients don't all have to use oxygen 24/7. Some with less severe cases only need the oxygen when they are exercizing or sleeping. Taking a spirometry test for lung function can determine if oxygen is needed or not. Those with less than 90% oxygen saturation in their lungs will need supplemental oxygen. Breathing may sap the strength of a COPD patient and they may lose muscle mass and can even become emaciated so they need more daily calories. A healthy diet of fruits and vegetables, and lean protein. This may also prevent malnutrition.
It is a good idea for the COPD patient to talk to their doctor about an exercise program tailored to their particular needs. Low impact exercise such as aerobic conditioning, light weight lifting, tread mill, stationary bikes, walking and swimming will help to strengthen the muscles in the lungs. They will want to build up endurance working slowly and sustain what they are able to do. When exercising outdoors they don't want the air to be too dry, too cold or too wet.
According to a 2009 study of the Journal of Cardiopulmonary Rehabilitation and Prevention those who practice deep breathing, power breathing, slow abdominal breathing experience less shortness of breath and increased oxygen absorption.It is recommended that COPD patients get a yearly flu shot, vaccine for pneumococcal infections and booster for pertussis (whooping cough).
Hot Galleries



Our Editor Reviews
Trending Story

Smell the Flowers
Peace and calm awaits as you take a walk in the garden. Nature's finest beckons as you caress the leaves of plants you pass by. Then, you see her. Dazzling, vibrant and beautiful. She may be surrounded by prickly thorns, protecting her like the king's guard. And to your eyes, she is unreachable, but your heart tells you to go nonetheless. You reach out to touch her, but the thorns pierce your skin. The pain heightens your senses, but you will yourself to bear the pain, you coax yourself to keep moving forward - to reach that goal. To reach her. You brave 10, 15, 20 more thorns. It hurts as you sweat under the heat of the sun. Finally, you do reach her. In your longing and in your weariness, you stop and just - just marvel at her beauty.
You gaze at her even as the sun scorches your back and your skin. In your mind you have already touched her. But you know that it would be a crime against nature to pluck her away from the one that nourished her into being. So then, you simply stop and smell the rose. New sensations from your olfactory senses fill your being with grace and joy. You knew that she could give you all those. Your lungs are filled with her essence and your self is filled with an epiphany of living. The smell of a rose coupled with the freshness of morning dew drops stuns you, nay, brings you to an ecstatic moment of calm. But you are a smoker.
Your lungs are a desolate battlefield, filled with scars and scorches, your mind is clouded and your ability to grasp the olfactory essence of a rose is hindered as many thousands of your nerves have been flayed and beaten by nicotine and hundred or so chemicals. Would you walk away from the rose upon realizing this truth? Having had the realization that you cannot appreciate it, you despair and just gaze at it. You sit down and watch and wait for a miracle to happen. You try to smell it again, this time, mustering with all your strength to breathe in stronger to try to suck in what fragrance you could. Still nothing. A tear makes it way down your cheek, as you live with the truth of your inadequate being. You wipe it away with your clenched fist as your body begins to shudder uncontrollably at the prospect of not being able to experience what she offers. Will this be your story? - - - -
- - - -
Creative Commons Image via Flickr